
At the DAAT conference in early September 2015 I heard the drug related death figures for 2014. Despite having warned people they would be worse than the previous year I was shocked and deeply saddened. I have waited to write this blog to get my thoughts together.
Last year I was shocked by the inaction of Government and many Local Authorities to the 2013 figures.
I was going to talk about the Naloxone Action Group, positive action by the Department of Health, questions in Parliament and early day motions on naloxone. I was going to talk about the fact that since the 2013 drug related death figures came out, I and so many others have worked to try and understand what is happening and the cause.
Personally I believe that increased heroin purity, poor heath and financial pressures on the drug treatment system are key factors in increasing drug related deaths. I also believe that action to increase naloxone availability in England will avert a significant proportion of these deaths. Without naloxone the figures would already have been, in my view, significantly higher.
However the 2014 figures are shocking to me, every death represents a person, perhaps a father or grandmother, certainly someone’s child, grief and the waste of a life. I picture the funerals as a silent rebuke to do more. The figures are the highest since records began.
As you read the statistics below, from the Office of National Statistics, take time to consider the people the figures represent.
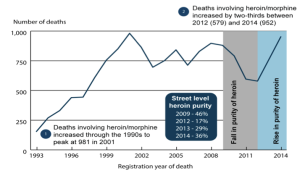
Heroin and morphine deaths rise by two-thirds in the past 2 years.

Within England, the North East has the highest mortality rate from drug misuse, London the lowest.

2014 registrations show drug related deaths reaching the highest level since records began.

Majority of heroin deaths were among the 30-49 year old age groups.

Males were over 2.5 times more likely to die from drug misuse than females.

Two issues seemed important to understand after the 2013 figures and they remain the same after the 2014 set. Firstly what is causing the rise in deaths? And secondly what is being done to prevent them?
A naloxone summit, hosted by Blenheim, bought together a campaign for a national naloxone programme in England. Through a FOI request we discovered the true extent of under provision of naloxone with only 32% of local authorities in England saying Naloxone was available. We formed the Naloxone Action Group England to ensure the regulations were changed, to ensure effective guidance was produced, and to ensure provision of naloxone across England. We got MPs to ask a range of questions in Parliament and gained support for an early day motion, sponsored by amongst others the current leader of the opposition Jeremy Corbyn and signed by the current Shadow Chancellor, John McDonald. This was not a party political issue; the EDM was also supported by current Conservative Minister Tracey Crouch. In total 32 MPs signed up to support wider naloxone availability.
Letters to the Minister from the Drug Alcohol and Justice Parliamentary group, chaired by Lord Ramsbotham secured firm assurance that the Government would make the changes recommended by ACMD to make naloxone more widely available from October this year.
Sadly, at the Naloxone Action Group we believe around 50% of local authorities continue to fail to provide naloxone. We will do a further FOI this year.
Meetings at Chatham House with senior officials revealed clear evidence that entering and leaving drug treatment and/or prison are particularly dangerous times for overdose and death. Thus pressure to leave treatment early and failure to adequately manage transfer of those with drug problems from residential settings could seriously endanger lives.
A drug related death summit held at the beginning of this year, hosted by Drugscope, Public Health England (PHE) and the Local Government Association, examined what might be causing the rise and to look at what might be done to reduce overdose deaths in future years. The attendees included policy makers from across government, commissioners, clinical and service provider leaders, and service user representatives.
The key messages from the summit were:
- The availability of accurate, timely and easily accessible data is important in order to make the appropriate adjustments to policy and practice in order to reduce drug-related deaths;
- The majority of drug misuse deaths still involve opiates, in particular heroin and methadone;
- Being in contact with a treatment service would appear to be a significant protective factor for drug-related deaths;
- Services and practitioners should pay attention to the elevated risk for those in treatment who are regularly overdosing, are drinking excessively, live alone in temporary accommodation or are homeless, or as a result of smoking-related diseases have compromised respiratory systems;
- Policy makers and commissioners should think about providing timely and accurate alerts to drug users who are not in the treatment system – including drug users who don’t use opiates;
- Commissioners and services should look at how they could supply naloxone more widely in the community to ensure those vulnerable to heroin overdose (including those not in treatment), their families, peers and carers are able to access the medicine.
Over the last year we have seen PHE nationally, clearly assert the need for action to reduce drug related harm and publish significant guidance on naloxone and reducing drug related deaths. However, at a time when drug related deaths are at their highest ever level, to cut £200million from Public Heath funding to local authorities is truly outrageous.
I am still ashamed to live in a country where things like the PHE £200 million cut happen at a time of evident need and many local authorities look the other way as people die as a result of the negligent failure to follow guidelines and supply naloxone.

Well said John.
Ken Stringer
Hi John, if purity is an issue how would you explain the fall in DRDs in Wales which is subject to the same market variations as England? More needs to be done urgently, we too said the figures would rise and agree that the lack of action is not acceptable. As a start I need figures for opiate deaths broken down on an annual basis for each LA area, this has been refused. I have some thoughts on what is happening
The changes from Oct 1 will help but don’t go far enough. Distribution and training needs to reach out to the wider population – families and in particular friends. They need access and also training.
Rises in opiate DRD usually have multi-factorial causes and alcohol is often implicated along with increased opiate intake over preceding days. There is good evidence to show that fluctuations and rises in purity alone is almost never the reason for fatal overdose. Long-term users especially have long coped with fluctuations in purity and have relatively good tolerance. Cutting agents in the UK are also not of the kind to produce overdose events. A good overview of cutting can be found here: http://www.cph.org.uk/wp-content/uploads/2012/08/cut-a-guide-to-the-adulterants-bulking-agents-and-other-contaminants-found-in-illicit-drugs.pdf